Endometrial ablation

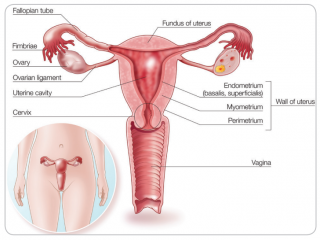
Endometrial ablation is a surgical procedure that removes the inside layer (the endometrium) or lining of the uterus. The endometrium is the part that sheds each month as a period (menstruation ).The endometrium consists of 2 parts:
1. A deep part (called the basalis)
2. A superficial part (called the superficialis)
Each month a thickening of cells occurs to produce the superficial part. In a usual menstrual cycle, where pregnancy does not occur and without any hormone treatments (such as the oral contraceptive pill), the superficial part is shed and menstruation occurs. The deep part is always present and does not shed to allow the process to be repeated in the following month.
 Sometimes, there may be excessive bleeding (causing clots, flooding and pain) at the time of menstruation. To find the cause of this bleeding, your doctor will take a history, perform a physical examination and perform or arrange tests, such as an ultrasound scan and taking a sample (biopsy) of the uterine lining.
Sometimes, there may be excessive bleeding (causing clots, flooding and pain) at the time of menstruation. To find the cause of this bleeding, your doctor will take a history, perform a physical examination and perform or arrange tests, such as an ultrasound scan and taking a sample (biopsy) of the uterine lining.
Heavy menstrual bleeding can be the result of a hormonal imbalance or changes, abnormalities within the uterus or bleeding disorders. Further information about heavy menstrual bleeding can be found on the RANZCOG website under patient information. One of the treatments available for this condition is endometrial ablation.
What are the outcomes following endometrial ablation?
The aim of any of the endometrial ablation procedures is to reduce menstrual blood flow (reduce periods). If you want to ensure
that there is no menstrual bleeding following treatment, then you should not choose an endometrial ablation and should discuss hysterectomy with your doctor as this is the only procedure that will guarantee no bleeding following the procedure. Following an endometrial ablation there are four possible outcomes:
1. No periods at all (called amenorrhea) (40% of cases)
2. Very light periods/spotting (40% of cases)
3. Reduced bleeding to what is acceptable (10% of cases)
4. No change in menstrual bleeding (10% of cases)
What happens in an endometrial ablation?
 Endometrial ablation can be performed using different methods. Scientific studies have not shown that one method is better than others, either in terms of outcomes or complications. The method recommended by your doctor will depend on your presenting symptoms, past history (such as a history of classical caesarean delivery) and other medical considerations (such as bleeding disorders). Other factors will include the type of ablation your doctor is familiar with and availability of specialised equipment.
Endometrial ablation can be performed using different methods. Scientific studies have not shown that one method is better than others, either in terms of outcomes or complications. The method recommended by your doctor will depend on your presenting symptoms, past history (such as a history of classical caesarean delivery) and other medical considerations (such as bleeding disorders). Other factors will include the type of ablation your doctor is familiar with and availability of specialised equipment.
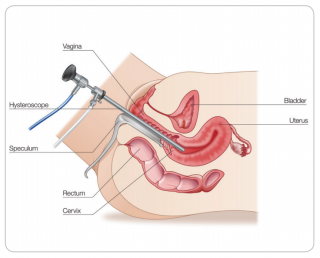
Generally, endometrial ablation is performed under a light general anaesthetic in a day-stay surgery or hospital. The initial steps are similar for all types of ablation. Your doctor may examine the inside of your uterus with a narrow telescope. This procedure is called a hysteroscopy may be performed before and/or after the procedure. Further information about hysteroscopy can be found on the RANZCOG website under patient information.
The next steps will depend on the type of ablation you are having. There are 4 kinds of ablation procedures performed in Australia and New Zealand.
Endometrial resection: following a hysteroscopy, a wire loop connected to an electrical current is attached to the hysteroscope.
The loop is about 4mm across and is used to cut strips from the endometrium until it has all been removed. During the procedure it is most important to remove both the superficial
and the deep parts of the endometrium to prevent regeneration of the endometrium occurring. Once the endometrium has been completely removed and the cavity is checked for any bleeding points the procedure is finished.
An advantage of this technique is that it can be performed at any time of the month, without specific preparation, since the lining layer is removed and the underlying muscle layer is easily identified. A disadvantage is that it requires the tissue to be cut, which may cause bleeding from the blood vessels in the muscle layer.
Endometrial rollerball ablation: in this method, the same procedures as for an endometrial resection are performed and the same effect achieved; however, instead of cutting through the endometrium, a special ball takes the place of the wire loop and an electrical current is passed through the endometrial lining to destroy it.
An advantage of this technique is that it does not require any cutting at all and therefore women who have conditions that affect their blood or are on blood thinning medication may benefit. It may be necessary to time the procedure to just after a menstrual cycle or have medication that will keep the endometrium thin if this is the procedure chosen.
Electrosurgical resection (NovaSure®) endometrial ablation: during this endometrial ablation a single-use sterile device is placed into the uterine cavity in a closed position and then opened out, a bit like a small and flattened umbrella. The surface of the device is wire mesh and this is attached to a generator that has
a suction device in it. The lining of the uterus is sucked onto the
wire mesh and an electric current is passed through the mesh. This destroys the entire endometrium.
Balloon (Cavaterm® or Thermablate®) endometrial ablation: during these procedures, a single use, sterile, deflated balloon is placed in the uterine cavity and this is filled with hot water or oil to transmit a thermal effect to the lining of the uterus to destroy it by heat. The entire surface is able to be destroyed by the heat.
What are the complications of endometrial ablation?
Complications relating to endometrial ablation may occur either:
1 During surgery (intra-operatively)
2 After surgery (post-operatively)
Intra-operative complications: these are rare, occurring in about 1/2500 cases. Some of the main risks include:
Accidental damage to the uterus where a perforation (hole) is made in the wall. If this occurs when there is no
 energy inside the uterus, then usually observation is all that is necessary. If this occurs during the procedure when any heating is taking place (during the active treatment phase) there is a possibility of damage to another organ and further surgery such as a laparoscopy (keyhole surgery) may be performed, or laparotomy (open surgery) to repair organs close by such as the bowel.
energy inside the uterus, then usually observation is all that is necessary. If this occurs during the procedure when any heating is taking place (during the active treatment phase) there is a possibility of damage to another organ and further surgery such as a laparoscopy (keyhole surgery) may be performed, or laparotomy (open surgery) to repair organs close by such as the bowel.
Other complications that may occur include heavy bleeding that may require an overnight admission, medications, or very rarely a blood transfusion.
For some types of endometrial ablation, fluid is used to allow vision of the uterine cavity. This fluid may be absorbed into the bloodstream through blood vessels that are opened during the removal of the endometrium. A unique complication of endometrial ablation using fluid is that excessive absorption of this fluid may lead to an imbalance in the blood salt levels, which may cause other complications, such as fluid on the lung or, rarely, on the brain. Monitoring fluid absorption with an automated device and stopping the surgery if the appropriate fluid level is reached will reduce this risk.
Post-operative complications: following surgery, it is normal to have vaginal bleeding for a few days to a week. Occasionally the bleeding or discharge may last for a few weeks as healing takes place. If there is an increasing amount of bleeding, bright blood loss, foul-smelling vaginal discharge or increasing pain then you should contact your doctor. Infections can occur and may require antibiotics. It is best to consult your doctor if you think that you have an infection following this procedure.
In the healing phase, it can take up to 6 months for your periods to settle. This is because the scarring that takes the place of the endometrium must form and stabilise. Should you have a heavy period following your endometrial ablation then this may be completely normal. It is the pattern over a period of time that will determine your final result. Very occasionally there can be an increase in the amount of pain that you may have that occurs either with vaginal bleeding (like period pain) or without bleeding. You should let your doctor know if this occurs. Treatment will depend on the cause, but may include taking pain medications, a simple procedure such as opening up the entrance to the uterus to let the blood out, or occasionally a hysterectomy.
The chance of you avoiding hysterectomy following an endometrial ablation in the long-term and for any reason is about 80%.
Endometrial ablation and fertility
It is still possible to get pregnant after an endometrial ablation, however it is very dangerous to both the mother and baby. Since the lining of the uterus is not able to support a pregnancy, there is also an increased chance of miscarriage or ectopic pregnancy. If the pregnancy does continue, there can be serious problems associated with the placenta such as the baby may be small due to poor blood flow of oxygen and nutrients. Endometrial ablation is therefore only suitable for women who have completed their family. You should not have an endometrial ablation if there is a chance that you may wish to have more children. Prior to the procedure, you should talk to your doctor about your choices for contraception which may include permanent contraception or sterilisation.
Frequently asked questions
How long will I have bleeding for after the procedure?
You are likely to bleed for approximately 48 hours following the procedure. There may be a red-brown discharge following this for up to 6 weeks. If you have pain, a foul smelling discharge or a discharge that is green-yellow you should contact your doctor.
 Will the procedure affect my sex-life?
Will the procedure affect my sex-life?
No, there are no changes to sexual function. In fact studies have shown that sexual function improves after endometrial ablation, presumably due to less inconvenience from heavy periods.
You can have sex as soon as the bleeding and discharge have stopped or after 4 weeks.
Will I go into early menopause?
No. Endometrial ablation does not affect the ovaries or the hormone levels. You will still have normal hormone function and will go through menopause at the normal time for you.
Is this a good procedure for pelvic pain?
This procedure is not intended as treatment for pelvic pain or painful periods. However, studies have shown endometrial ablation is not only likely to reduce the heaviness of your periods, but may also reduce the amount of pain that you suffer experience with your period.
What will happen to my PMT?
Premenstrual tension (PMT) or pre-menstrual syndrome (PMS) is a combination of symptoms. It is unclear as to why it occurs and treatments are variably successful. Studies have shown that PMT symptoms are significantly reduced following endometrial ablation; however, it is not recommended as a primary treatment for these problems.
What happens if the procedure is not successful?
Endometrial ablation will not be successful in about 10% of cases. In this situation, options may include medications, repeat ablation (by the resection or rollerball techniques only – all other methods are unable to be used a second time) or hysterectomy. Hysterectomy following an endometrial ablation may be for failure of the treatment, or the development of a new problem, such as a fibroid or pain. You should discuss these alternatives with your doctor.
Can I have an endometrial ablation if I have had a caesarean delivery?
Yes. If you have had a usual caesarean (lower segment incision) any of the endometrial ablation treatments are suitable for you.
If you have had a classical caesarean (an up and down incision), then you should not have the NovaSure, Cavaterm or Thermablate procedures. The other procedures are possible and you should discuss this with your doctor further.
What if I am menstruating at the time of my procedure?
The timing of your cycle is not critical for resection or NovaSure. For the other techniques, it is optimal to perform the procedure in the first week after your period has finished, or use a simple medication to thin the lining before the treatment.
When will I know if the procedure has been successful?
It takes between 3 and 6 months for the scarring of the uterine lining to become effective. Therefore, it is possible that you may have heavy periods initially, though these become lighter as time progresses.
What if I have fibroids or polyps?
A fibroid is a non-cancerous tumour that grows in the wall of the uterus. A polyp is a growth in the lining of the uterus. If you have fibroids or polyps, then these may be removed at the time of an ablation and
will be sent for testing. If you do have fibroids or polyps and heavy bleeding, then the diagnosis termed abnormal uterine bleeding polyp or leiomyoma (fibroid) is made and you should ask your doctor about specific management for these.