Mirena_HCP_Brochure Product Information


What is Mirena®?
Figure 1. Schematic presentation showing the localised release of levonorgestrel from Mirena® into the uterine cavity
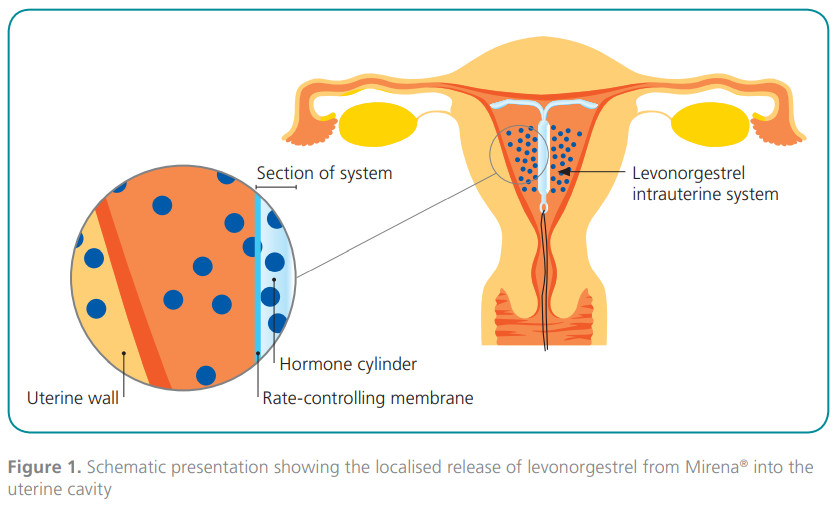
Mirena® is a hormone-releasing intrauterine contraceptive system. It consists of a small T-shaped plastic frame with a steroid reservoir surrounding the vertical stem. After placement into the uterus, Mirena® releases small amounts (initially 20mcg/ day) of the progestogen levonorgestrel into the uterine cavity (Figure 1). Mirena® provides effective contraceptive protection for up to five years, after which it must
be replaced or removed.
How does Mirena® work?
The contraceptive and therapeutic effects of Mirena® are based on the local effects of levonorgestrel in the uterine cavity:
Thickening of the cervical mucus, which inhibits passage of sperm through the cervical canal (Barbosa et al. 1990, Lewis et al. 2010).
Inhibition of sperm motility and function inside the uterus and the fallopian tubes, preventing fertilization (Videla-Rivero et al. 1987).
Prevention of endometrial proliferation (Silverberg et al. 1986).
Initially, ovulation may be inhibited in some users. It is important to note that because of the mechanisms of action, Mirena® cannot be considered an abortifacient (a common misconception).
How reliable is Mirena®?
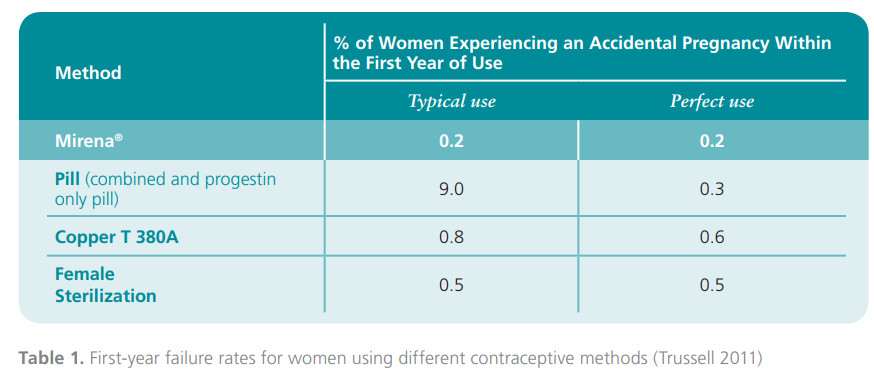
Mirena® provides high contraceptive reliability: the first-year failure rate is 0.2% and the cumulative failure rate at 5 years is only 0.7% (Mirena Product Monograph 2010). This degree of contraceptive efficacy is comparable with that of female sterilization (Table 1). Moreover, fertility returns immediately after removal of Mirena®.
The number of ectopic pregnancies has been remarkably low, the incidence being approximately 0,1% per year, considerably lower than in women using no contraception (0.3–0.5 per year) (Mirena Product Monograph 2010).
Who should use Mirena®?
 Mirena® is an ideal option for women looking for reliable long-acting contraception.
Mirena® is an ideal option for women looking for reliable long-acting contraception.
Mirena® is a suitable method for women who prefer light and scanty periods and effective contraception. Women with regular but heavy periods (idiopathic menorrhagia) may be recommended to use Mirena®, since it will also reduce their menstrual blood loss effectively, by 86% at three months of use and by up to 97% after one year of use (Andersson and Rybo 1990; Milsom et al. 1991). The decrease in menstrual blood loss is accompanied by
increased hemoglobin and ferritin levels, thereby reducing the likelihood of anemia in women with heavy menstrual blood loss. Concomitantly, dysmenorrhea is alleviated.
Who should not use Mirena®?
Women with the following conditions and diseases should not use Mirena®: known or suspected pregnancy; untreated genital infection; confirmed or suspected uterine or cervical malignancy; undiagnosed abnormal uterine bleeding; congenital or acquired uterine anomaly (including fibroids if they distort the uterine cavity); acute liver disease or liver tumor; progestogen-dependent tumors.
Although the risk of pelvic inflammatory disease with Mirena® is low (Andersson et al. 1994), care should be taken to avoid insertions in women at high risk of sexually transmitted diseases in order to minimize the risk of pelvic inflammatory disease.
Bleeding pattern changes with Mirena®
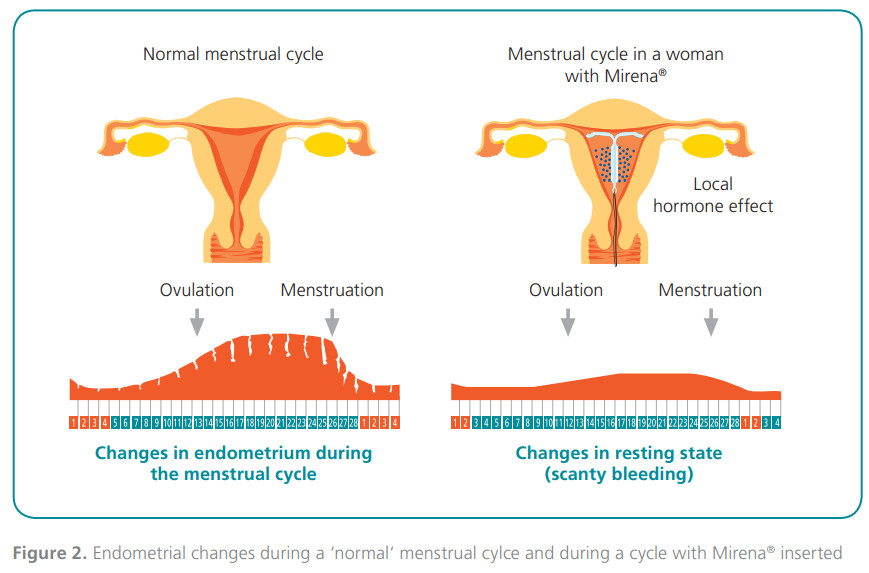
Due to the local action of levonorgestrel on the endometrium (Figure 2), all women will experience a change in their menstrual pattern. During the first few months of use, there is often frequent irregular bleeding or spotting (Nilsson et al. 1980; Heikkila et al. 1982), but the volume of blood loss is reduced compared with normal menstruation (Andersson and Rybo 1990; Milsom et al. 1991). The number of days with spotting or bleeding decrease gradually (Nilsson et al. 1980;
Heikkila et al. 1982). At the end of the first year of use, menstrual blood loss is drastically reduced and some 20–60% of women experience total absence of bleeding (amenorrhea) (Xiao et al. 1995; Suvisaari and Lahteenmaki 1996; Hidalgo et al. 2002).
The role of counseling
Adequate and effective counseling about the anticipated changes in menstrual bleeding and the underlying cause for these changes will help improve patient satisfaction with Mirena® as well as improve continuation rates by avoiding unnecessary removals (Davie et al. 1996).
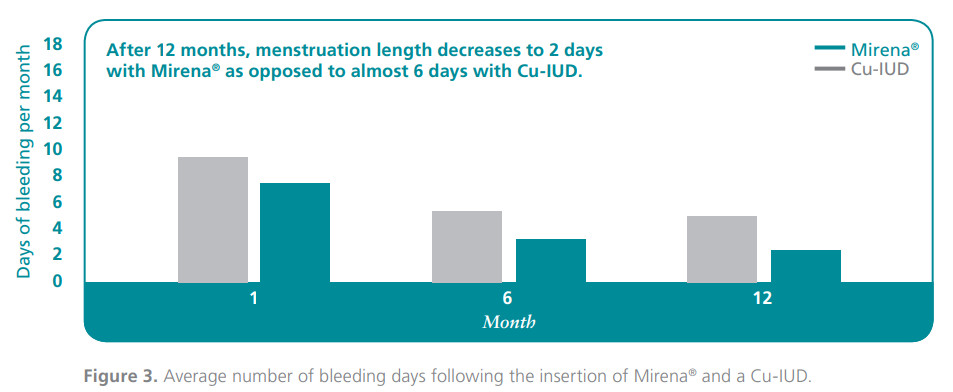
Women should be counseled to differentiate between bleeding and spotting. Understanding that irregular spotting is usually a short-term problem during the initial months of use can help motivate continuation of use. In addition, women should also be reassured that the absence of bleeding or the presence of scant bleeding are not signs of pregnancy or disturbed ovarian function. Indeed, a survey of Mirena® users in clinical practice showed that total or occasional absence of menstruation was strongly associated with high patient satisfaction and continuation (Backman et al. 2000). The bleeding profile with Mirena® is quite different from that of Copper intrauterine devices, which frequently increase bleeding, whereas Mirena® decreases it (Figure 3).
Safety profile of Mirena®
Hormonal adverse effects are mild and generally transient in nature, since the action of Mirena® is mainly local. Most commonly reported adverse effects include lower abdominal pain, acne or other skin problems, back pain, mastalgia,
headache, vaginal discharge, mood changes and nausea. These adverse effects are mostly reported at the beginning of treatment (Andersson et al. 1994).
Serious adverse effects are rare. Partial or total perforation (penetration of the wall of the uterus or cervix) may occur in less than 1 in 1,000 users, most often during insertion. If perforation occurs, the system must be removed as soon as possible.
The risk of pelvic infection is increased during the first month after insertion of intrauterine devices.
Bleeding pattern changes with Mirena®?
Although the initial cost of Mirena® itself may seem high (initial up-front payment in countries where is not reimbursed or there is no co-payment), when used
over its prescription lifetime of 5 years it has lower total method costs and better effectiveness compared with oral and barrier contraceptive methods. As such, Mirena® is one of the most cost-effective long-acting contraceptives available.
Although hysterectomy is considered the ultimate treatment for menorrhagia, Mirena® offers potential cost-benefits compared with hysterectomy in the treatment of menorrhagia. The total costs arising from healthcare and productivity losses were shown to be about 3-fold lower with Mirena® than after hysterectomy over the 12 months of treatment and still 40% lower at 5 years (Hurskainen etal. 2001; Hurskainen et al. 2004). Moreover, Mirena® has been shown to improve quality of life scores, general and psychological health parameters, and hemoglobin and ferritin levels to a similar extent as hysterectomy (Hurskainen et al. 2001).
Importantly, Mirena® provides effective treatment of menorrhagia while preserving future fertility and avoiding of the risks associated with a surgical procedure.
Summary
- Mirena® is a highly effective contraceptive, comparable with sterilization
- Mirena® is an ideal option for women who are looking for long-acting
- contraception or those with idiopathic menorrhagia
- Mirena® reduces the duration and the amount of menstrual bleeding
- Mirena® is one of the most cost-effective long-acting contraceptives avail
References:
Andersson K, Odlind V, Rybo G (1994) Levonorgestrel- releasing and copperreleasing (Nova T) IUDs during five years of use: a randomized comparativetrial. Contraception 49:56-72
Andersson K, Rybo G (1990) Levonorgestrel-releasing intrauterine device in the treatment of menorrhagia. BJOG 97:609-694
Backman T, Huhtala S, Blom T et al. (2000) Length of use and symptoms associated with premature removal of the levonorgestrel intrauterine system: a nation-wide study of 17,360 users. BJOG 107:335-339
Backman T, Rauramo I, Huhtala S, Koskenvuo M (2004) Pregnancy during the use of levonorgestrel intrauterine system. Am J Obstet Gynecol 190: 50-54
Barbosa I, Bakos O, Olsson SE, Odlind V, Johansson ED (1990) Ovarian function during use of a levonorgestrel- releasing IUD. Contraception 42: 51-66
Chiou CF, Trussell J, Reyes E et al. (2003) Economic ana- lysis of contraceptives for women. Contraception 68:3-10 Davie JE, Walling MR, Mansour DJ et al. (1996) Impact of patient counseling on acceptance of the levonorgestrel implant contraceptive in the United Kingdom. Clin Ther 18:150-159
Heikkila M, Nylander P, Luukkainen T (1982) Body iron stores and patterns of bleeding after insertion of a levon- orgestrel- or a copper-releasing intrauterine contraceptive device. Contraception 26:465-474
Hidalgo M, Bahamondes L, Perrotti M et al. (2002) Blee- ding patterns and clinical performance of the levonorgest- rel-releasing intrauterine system (Mirena) up to two years. Contraception 65:129-132
Hurskainen R, Teperi J, Rissanen P et al. (2001) Quality of life and costeffectiveness of levonorgestrel-releasing intrauterine system versus hysterectomy for treatment of menorrhagia: a randomised trial. Lancet 357:273-277
Hurskainen R, Teperi J, Rissanen P et al. (2004) Clini- cal outcomes and costs with the levonorgestrel-releasing intrauterine system or hysterectomy for treatment of menorrhagia: randomized trial 5-year follow-up. JAMA 291:1456-1463
Milsom I, Andersson K, Andersch B, Rybo G (1991)
A comparison of flurbiprofen, tranexamic acid, and a levonorgestrel-releasing intrauterine contraceptive device in the treatment of idiopathic menorrhagia. Am J Obstet Gynecol 164:879-883
Mirena Product Monograph, 9th Edition, 2010
Nilsson CG, Lahteenmaki P, Luukkainen T (1980) Pat- terns of ovulation and bleeding with a low levonorgestrel- releasing intrauterine device. Contraception 21:155-164 Nilsson CG, Lahteenmaki PL, Luukkainen T (1984) Ovarian function in amenorrheic and menstruating users of a levonorgestrel-releasing intrauterine device. Fertil Steril 41:52-55 Schering AG (2006) Mirena Prescribing Information.
Silverberg SG, Haukkamaa M, Arko H, Nilsson CG, Lu- ukkainen T (1986) Endometrial morphology during long- acting use of levonorgestrel-releasing intrauterine devices. Int J Gynecol Pathol 5:235-241
Suvisaari J, Lahteenmaki P (1996) Detailed analysis of menstrual bleeding patterns after postmenstrual and posta- bortal placement of a copper IUD or
a levonorgestrel-releasing intrauterine system. Contracepti- on 54:201-208
Trussell J (2011) Contraceptive failure in the United States. Contraception 83:397-404, 2011
Xiao B, Zeng T, Wu S, Sun H, Xiao N (1995) Effect of levonorgestrel-releasing intrauterine device on hormonal profile and menstrual pattern after longacting use. Contra- ception 51:359-365
SPC available at the booth and the download station.

Bayer Pharma AG
Strategic Marketing General Medicine 13342 Berlin, Germany
www.bayerpharma.com
©2012, Bayer Pharma AG. All rights reserved.
Mirena® product description: Mirena® is a levonorgestrel-releasing intrauterine system (IUS) with an initial release rate of 20 microgram/24 h. Mirena® is effective for five years. Indications: Contraception, idiopathic menorrhagia, and protection from endometrial hyperplasia during estrogen replacement therapy. Contraindications: Known or suspected pregnancy, current or recurrent pelvic inflammatory disease, lower genital tract infection, postpartum endometritis, infected abortion during the past three month, cervicitis, cervical dysplasia, uterine or cervical malignancy, progesterone-dependent tumors, undiagnosed abnormal uterine bleeding, congenital or acquired uterine anomaly including fibroids if they distort the uterine cavity, conditions associated with increased susceptibility to infections, acute liver disease or liver tumor, hypersensitivity to the constituents of the preparation. For full product information see package insert. For further information please contact the Manufacturer Bayer Pharma AG, D-13342 Berlin, Germany, or on the Internet: www.bayerpharma.de, or your local country office. This information is based on the CCDS/Version14/March 22, 2011.
www.bayerpharma.com www.mirena.com